My family has been going through it the past couple weeks. It’s just more of the same 2020 nonsense that everyone is experiencing, but that doesn’t make it any easier. I’ve been thinking about a post on executive functioning, as I can imagine we’re all working a little harder on this skill of late, but also because I recently ran across something that might help our kids be a little more effectual with a lot less work and frustration.
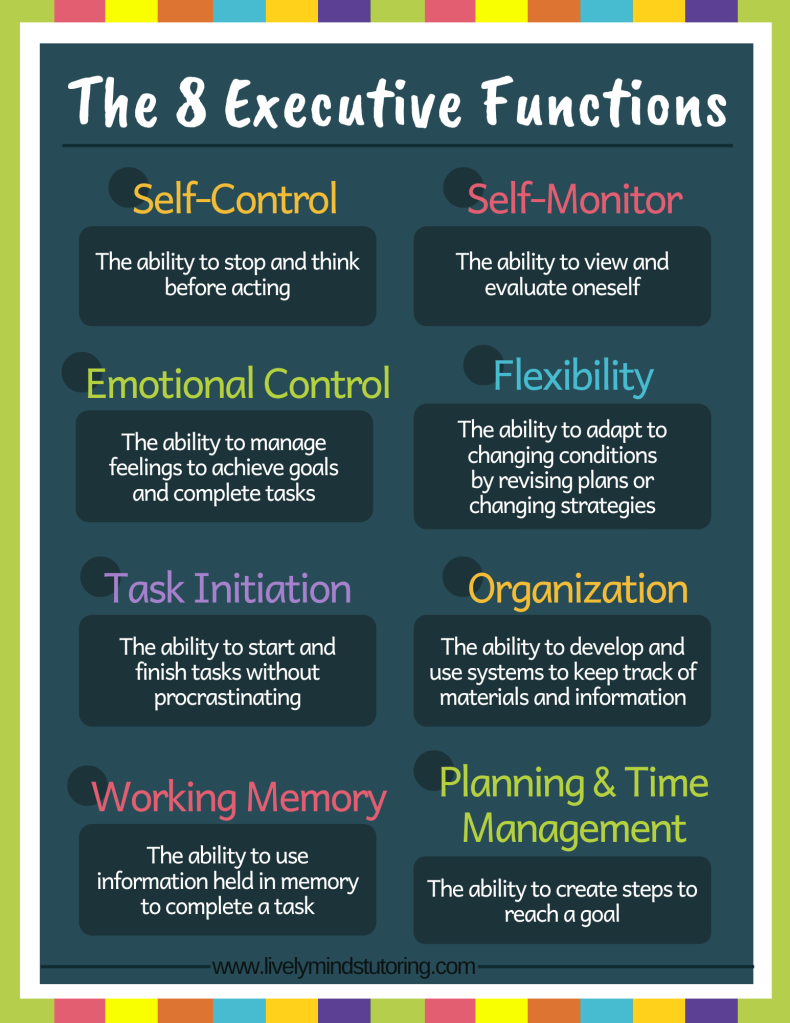
Executive function is the term for the overall management of the brain. It is what allows us to prioritize tasks and get things done and it involves three overarching areas: working memory, cognitive flexibility, and inhibitory control (including self-control). The eight executive functions are self-control, self-monitoring, emotional control, flexibility, task initiation, organization, working memory, and planning & time management.
There are many brain differences that impact executive functioning including things like autism, ADHD, depression, and trauma to the brain. And, if you’ve spent time around kids, you’ll recognize that their executive functioning is still under construction. In fact, executive function develops all the way into adulthood. Kids who are struggling with it might not be able to pay attention, hold onto a series of instructions, transition from one task to the next, or plan out action steps. As a child, I had many, many hours of therapy to help me improve my executive functioning skills, so I was intrigued when I recently ran across a strategy that promises improvements in executive function.
Kristen Jacobsen (MS CCC-SLP) and Sarah Ward (MS CCC-SLP) are two speech language pathologists who have been studying executive function for the past 20+ years and now co-direct Cognitive Connections, a specialty practice in Massachusetts. Together, they created the 360 Thinking™ Executive Function Program that includes a strategy developed by Sarah Ward called Get Ready, Do, Done. This strategy coaches children to identify what needs to be done at a future time, imagine what “done” looks like, work backward to plan out the steps to get there, and then collect needed materials to accomplish the task. It is a way to lay out each step for those whose brains don’t automatically do the planning for them. The model plans backward before taking steps forward.
What will it look like when I am done?
What steps do I need to take to be done? How long will each step take?
What do I need to get ready?
What materials do I need to do the steps?
Time to do the task. Create a timeline and time markers.
When I was little, I used to get frustrated to the point of shutting down when I was told to clean my room. In childist terms, I might have been called lazy or stubborn, but the problem I had was that I simply didn’t know what to do! I needed someone to show me my room clean and straight several times, so I’d have the picture in my mind. I needed to be walked around the room and shown where each item was supposed to go. I needed a step-by-step plan, like:
Get cleaning supplies.
Clear off and make the bed to use as a staging area if needed.
Pick up and put away items from the floor as follows: trash, dishes, clothes, toys, books, and everything else.
Organize wardrobe and trunk.
Wipe dust and grime from surfaces.
Clean glass.
Sweep floor.
That never happened for me. I stumbled through housework until well into adulthood when I came across the organizing and cleaning industries and learned how to properly do housework. Even with small children now, I’m able to keep my house nice and clean. I even put laundry away after it’s dried, which is something I never did as a young adult. Check out this quick video that uses cleaning a room to explain executive functioning:
If you’d like to give Get Ready, Do, Done a try, check out these free resources:
Months ago, a therapist friend shared with me a page out of a strategic family therapy textbook that looked at how a family’s response to challenging behaviors determines whether the behavior will be resolved or become a problem. The author gave an example of a boy who became temperamental after the birth of his baby sister. His father punished him to stop the behavior, but that punishment served to confirm to this child that his parents loved his sister more than they loved him. His behavior intensified and the punishment followed suit. There was no resolution. In this case, his father saw only one explanation for the behavior: that the child was insolent and disrespectful. He did not imagine that his son was crying out for love and compassion.
In this chapter of the book, the author introduced the idea of Order of Change, which refers to the ways in which a system can change. So much of what we can use to shift the ambit of entire organizations also works for families. It makes sense. Families are organizations composed of people as well. The book detailed two orders of change, but I will include a third to present more options. Important note: The progression from first to third, DOES NOT INDICATE a progression in value. Any one of these might be appropriate in a given circumstance.
First Order Change: Maintains existing structure and uses increases and decreases to restore balance. The goal here is not to change the basis of the system, but to improve upon it. First Order Change is Transactional.
Second Order Change: Revolutionizes how the system functions altogether. The goal here is to change the system where it needs to be altered to work better. Second Order Change is Transformational.
Third Order Change: Tosses the system out the door altogether and encourages members of the system to become aware of system inconsistencies and dysfunction, question approaches, and take democratic steps toward improvement. The goal here is to increase awareness of the issues and buy-in from the participants in the system. Third Order Change is Innovative.
My first thought as I re-read this now, as so many of us are dealing with how we will send our children to school, is that the three orders seem to align with alternatives to the educational status quo. What better way to explain systems change than through something we’re all wrestling with. Let’s consider the catalyst to be the need to protect student health and see what each option provides.
First, there’s revamped brick and mortar school and school-at-home, e-school, or virtual school, whatever your school system might be calling it. Whether your child goes to school in person or stays at home and completes work there, this option packages school into a solution that allows parents to make decisions based on their comfort level with the school’s safety plan while maintaining the expected educational trajectory. For many families, especially those in which the adults don’t have a lot of time at home or are experiencing health issues, maintaining familiarity and taking advantage of the existing system makes sense. The new safety plans and hybrid or virtual options are an example of a first order change that prioritizes the health of the students by making incremental adjustments to the system.
Second, there’s homeschooling. Many options exist wherein an adult teaches a child at home outside the auspices of a brick and mortar school. Each of these echoes the familiar schooling system, but apply revolutionary changes to the schooling approach, the curriculum, the schedule, and so on. Many, many families have withdrawn their children from the school system this fall and have embarked upon the journey of “COVID Homeschooling” which will presumably end when the threat is no more. Some of these folks, like my family, will continue homeschooling for the foreseeable future. This option makes major alterations to the system to prioritize the health of the students.
Third, there’s unschooling. If ever there were a great example of Third Order Change, this is it. Haven’t heard of unschooling? It loosely falls under the umbrella of homeschooling, but it is truly innovative. Learning is completely student-led. Parents don’t teach unless their assistance is requested. Instead, they seek to create opportunity for their children to engage with their areas of interest. There is no curriculum. There is no hard and fast schedule. There is only the natural curiosity of the child being supported by an observant adult. Unschooling is democratic and deeply respectful of children. Personally, I would consider it the most anti-childist educational option for children.
Applying Order of Change Every Day
I offer this information about Order of Change neither to make you feel inadequate nor to overwhelm you, but to present a proposal for addressing challenging behaviors from your perfectly reasonable children. So often, our reactions to our children’s behavior fan the flame instead of creating space for connection.
Take, punishment, for example. Why do parents punish their kids? Because it works… in the short-term. It doesn’t change behavior. It stops unwanted behavior in the present, but does nothing to impact the moral development of the child. Punishment is an example of a First Order Change strategy. It uses the existing paradigm to make a small adjustment to bring the child back into alignment with comfortable expectations. The truth is that many children have grown into functional adults under this paradigm. The trouble is that we can’t know how much better a person’s quality of life might have been had they been given opportunity to learn, grow, and connect with their parents.
That’s why we, as Peaceful Parents, must recognize that we’re not simply working toward raising kind and respectful children. We’re also working toward giving our children the gift of positive self-image, the ability to work through times of struggle, and such intimate knowledge of themselves that they will recognize when they need extra help to sustain their mental health. Peaceful Parents tend toward Second and Third Order change when it comes to discipline for these reasons. We see that the existing system is childist and often cruel and we look for ways to humanize and elevate our kids. There is great value in First Order Change once we’ve built for ourselves an anti-oppressive system. Until then, it is up to us to question the whys and the hows of the way our culture approaches childlikeness.
Did y’all see the study from November 2019 that found screen use greater than the amount recommended by the American Academy of Pediatrics was associated with decreased microstructural organization and myelination of brain white matter tracts that support language and emergent literacy skills? Big yikes! Does that mean screens cause brain damage? That’s certainly a question I’ve seen floating around the internet. Parents are rightfully concerned about screen time when study after study shows these terrible outcomes.
There’s that 2013 literature review on screen time use in children under the age of three. Bad news.
And, that 2015 literature review on the effects of screen time on children’s sleep found. Terrible stuff.
And, that 2018 literature review on the physiological and psychological effects of screentime. You might as well just give up at this point.
And, that whole Research Roundup that seems to exist to fill parents with dread. Oh, the horror!
But, check this out.
The 2013 review found that there is very little research on infants and toddlers and that more research is needed to better understand the environmental, socio-cultural, and behavioral correlates for young children.
The 2015 review found that none of the studies they looked at from 1999-2014 could establish a causal connection, measurement errors of screen time exposure and sleep limited the outcomes of the studies, and factors like characteristics and content of screens was not well understood.
And, the 2018 review found that psychophysiological resilience in children requires the ability to focus, good social coping and attachment, and good physical health all of which could be impacted by “excessive” digital media use. They further recommend more research on duration, content, after-dark use, media type, and number of devices.
In fact, there’s a 2015 literature review on the association of parental influences with physical activity and screen time among young children found that there is a causal connection between the parents’ physical activity and screen use and that of the children. It should come as no surprise that the behavior of parents directly influences the behavior of their children.
And, that first study I mentioned? The one from 2019 about how screens change the brains of little kids? If you look a little deeper, you’ll see that the sample size is both small and homogenous and that the survey and testing scores used in the study did not meet the threshold for statistical significance when income was included in the model. Those details change the story a bit.
Minding the Nuance
The reality is that there is valuable research happening, but we simply don’t understand what’s really going on. That’s why the pediatric organizations that exist to protect our kids are sounding the alarm. They’re saying look at all this data we’re seeing! Something is happening. Pay attention. So, if your family’s lifestyle flows better without any screens, by all means, do what works for you. This post is for those of you who want to incorporate screens without fear.
There are some things we can discern intuitively about screen use.
It can be distracting. Background sounds from a TV at low volume add static to the environment where infants and toddlers play. A measurable impact has been found on the ability of very small children to develop play skills naturally when TVs are used as noise fillers.
It can signal trouble. While we don’t know that screens cause depression, we do know that children who watch a lot of TV often have clinical depression that necessitates medication. So, it’s worth paying attention to what your kids are doing, so that you can intervene if necessary.
It can replace other healthful behaviors. A child who is watching TV or playing video games is not outside running around. And, a child who is watching TV or playing video games is not telling you about the troubles they’re having.
Now, something that doesn’t get enough air time in these discussions is the economics of restriction. Essentially, by restricting a thing, we increase its value. As explained by Pam Sorooshian, unschooler extraordinaire,
When you only allow a limited amount of TV, then the marginal utility of a little more tv is high and every other option looks like a poor one, comparatively. Watching more TV becomes the focus of the person’s thinking, since the marginal utility is so high. Relax the constraints and, after a period of adjustment and experimentation to determine accurate marginal utilities, the focus on TV will disappear and it will become just another option.
The more you restrict, the more they’ll crave screens. It can feel uncomfortable to loosen the reins and it’s pretty likely your child will consume seemingly impossible amounts of flickering deliciousness at first. But, over time, and in the presence of intentional investment in your child’s needs and wants, screens will lose their luster and become just another activity.
If you’ve been restricting your child’s screen time, because you wanted to do the best possible thing for them or because you felt their screen use was getting out of control, it’s ok. You’re not alone. Not by any means. Just know there is an approach to screen use that is responsible and respectful, whenever you’re ready.
Anti-Childist Screen Use Monitoring
One of the things about the furor over screens that particularly bothers me is the emphasis on cognition and school performance. We’re encouraged to limit our children to a screen schedule of our making, so they can possibly do better in school at some point in the future. But why? Why is academic success the measure of a good life? Why are we not prioritizing our children’s ability to regulate their own behaviors and activities by giving them ownership over the way they choose to spend their time?
We can trust our children to make good decisions when we set them up for success. In our house, I try to limit my compulsion to set rules for everyone. Whenever my kids want to watch TV, I’m ok with it. They have free access to their tablets to use as they wish. But, I also create an environment where they don’t have any desire to obsessively consume that visual stimulation. We spend lots of time outside. We read. We do chores. We play, craft, and bake together. When I see one of my kids struggling to transition from screens to another activity, I intervene. When that happens, it means there’s something deeper going on that needs to be addressed. It doesn’t mean I need to arbitrarily limit screen time. I have some guidelines for my family in the back of my mind to help ensure that I’m providing the most effective mix of activities and the best possible education around the use of screens.
Be Intentional. Consider using screens on purpose. That means avoiding the use of TVs as background noise and trying not to hand your kids screens to keep them occupied. Instead, let your children decide when they want to use screens and for how long. And, have them choose one screen at a time. In general, our TV doesn’t get turned on until 3 PM, if at all. There’s too much other fun stuff to do.
Be Interactive. Studies show that children can learn a great deal from interactive touchscreens when their parents help them and reinforce what they’re learning.
Be Wise. Particularly when it comes to older kids, parents need to prepare children for the risks of predators and dangerous malware. Talk to your kids about these dangers and make a plan together for how to stay safe.
Choose Educational Content. Programs like Sesame Street and Daniel Tiger provide important information and skills to little kids, especially when families reinforce in daily life what the kids are learning online.
Eat Without Distraction. One rule we do have is that our dining table is a toy-free, screen-free space when we’re having a meal. It’s a matter of mutual respect and consideration. Family meals are sacred in my house. They’re one of the few opportunities we have to get together and chat over one of the most fundamental human activities.
Get Plenty of Fresh Air and Exercise. Getting outside is so important for every member of the family, but especially children. They need lots and lots of movement throughout the day to improve focus, digestion, motor skills, and sleep. Rather than restricting screens, think about encouraging more movement for balance.
Practice Good Sleep Hygiene. The so-called warnings about blue light got a little kick in the pants this year. A study challenged the idea that blue light impacts circadian rhythms. We don’t actually know if blue light is a problem. What we do know is that stimulation of any kind interrupts our sleep cycle. In our house, all screens and radios go off at 6:30 pm. That’s our family time and we cherish the ability to interact with each other without distraction. For a great night’s sleep, keep your kids’ room very dark, relatively cool (65 to 68 degrees Fahrenheit), and comfortably quiet.
Like many parents, when I first became a mom, I was hypervigilant about everything. I stressed myself out trying to do everything by the book, until life taught me that wisdom beats out perfection every time. If you want your children to enjoy screens, let them. Formulate some guidelines for yourself and conduct self-checks to make sure your guidelines are working. Talk with your kids about your concerns. Let them know your values and also that you trust them to know what their minds and bodies need. As new evidence emerges, we’ll be in a great position to shift some of our guidelines to better support our children’s development. Screens are ok, y’all. Promise!
Ever have moments when you feel like you’re in sync with your kids and things are amazing? If so, did you know you can have even more of those moments? Kids do well when they can, and you can help them out by understanding better where they’re coming from.
Marriage and Family Therapist, Galyn Burke, put together a fantastic resource on the way children’s brains develop. She explains that the three major parts of the brain (hindbrain, midbrain, and forebrain) develop on different timelines. They have to. Our brains are complex with high energy demands. It takes a while to get everything in order.
The reptilian hindbrain looks like someone dropped a crocodile brain into our heads. This part of the brain serves the most basic purposes including regulating autonomic functions like breathing and instictive behaviors like threat patrol.
The limbic midbrain is our emotion center. It’s what allows us to be empathetic, social creatures. This is the part of the brain where children process their world.
The neocortex forebrain is where our rational mind lives. This part doesn’t fully develop until the mid-20s in humans. We like to think of this area as the logic center, but without the midbrain, our logic is incomplete.
Childhood is an incredibly crucial time in the life of a human being when we learn how to be human. We figure out what emotions are and how to work with them. We learn how to love each other and respect boundaries. And, we learn our personal signs of dysregulation and how to cope. If children are not treated gently and responsively, any of these skills can be hindered.
So, you know that brain development isn’t as simple as 1, 2, 3, but did you know that even babies can think logically before they can talk? Turns out, our ability to reason doesn’t depend on language or understanding. A study that came out a few years back found that preverbal infants notice when something is wrong and try to work out a solution. The scientists figured out that “at the moment of a potential deduction, infants’ pupils dilated, and their eyes moved toward the ambiguous object when inferences could be computed, in contrast to transparent scenes not requiring inferences to identify the object. These oculomotor markers resembled those of adults inspecting similar scenes, suggesting that intuitive and stable logical structures involved in the interpretation of dynamic scenes may be part of the fabric of the human mind.” And our ability to reason explodes from that point.
Alison Gopnik, Professor of Psychology and Affiliate Professor of Philosopy at the University of California at Berkeley and author of The Gardener and the Carpenter, has been studying children for a long time. What she has found is that children have a greater capacity for innovation and creativity than college students all while applying clear logic. She explains that 3-year-olds will offer a stream of consciousness when asked to give us their thoughts, but if you use their own language to ask them concrete questions, the responses will be sensible and surprising.
Check out this piece explaining some of her experiments. You might just find something useful (Hint: Don’t miss the part where the researcher notes that having children explain something themselves increases their understanding of it.)
Now that you know just how brilliant your child is and you know why they can appear to be illogical, you might be surprised to learn that a very simple solution can flip a switch for your child. When a child’s limbic system is on overload, top to bottom exercises can be useful. These are exercises that require movement across both the top and bottom parts of the body. Things like standing stretches and light weight lifting can help your child’s brain regulate itself.
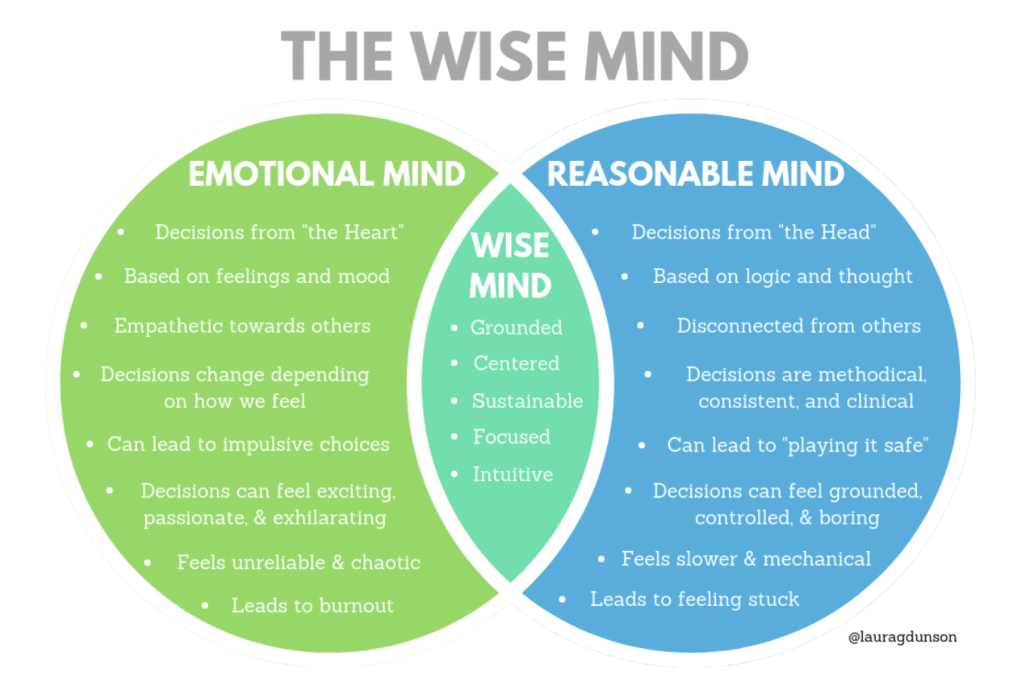
One final thought that comes to mind is Dialectical Behavior Therapy (DBT) with its focus on integration. In DBT, there exists a concept of the Wise Mind, which is “the balanced part of us that comprises our inner knowledge and intuition, where our emotional thinking mind (thoughts driven by distressing feelings) and rational thinking mind come together, the part of us that just ‘knows’ that true reality.”
Many adults need therapeutic intervention to learn to live into their Wise Mind. Children, whose brains are still forming, need direction and practice to find this place. When you recognize that your children are logical, but not logical in the exact same way that you are, it can become easier to learn to speak their language and to offer responses that help them integrate all the parts of their brains. I firmly believe that children are perfectly reasonable and I hope that, now, you do too.
Have you ever heard the term __________ People Time to refer to someone running late? That blank could refer to Black people, Latinx people, or any number of other cultures. Do you know why it’s a thing in the first place? Because of something called “time orientation.” Some cultures don’t have any real investment in the passage of time, some are polychronic, and some are monochronic. Perhaps, unsurprising, it’s been theorized that the less concerned people are about time, the warmer the climate in the culture’s ancient past. The idea is that inhabitants of warmer climates, historically, had to concern themselves less with clothing and food than did inhabitants of colder climates who spent more time on basic survival. If you have a short growing season and a long winter, time will feel in very short supply.
Polychronic cultures are those in which people are lax about time. Their focus in on community and relationships and they value things like relaxation. Monochronic cultures are centered around time and schedules. They work through time in a linear direction and they value things like promptness. So, when I tell you that predominantly white cultures are primarily monochronic, including the colonizers who settled in the United States and built a culture around their values, does it come as a shock? Probably not. Fast-forward to today and people from historically polychronic cultures are made to feel that they are wrong for being late or for talking for too long or for assuming context or for interrupting. However, they aren’t wrong. They’re just different.
The characteristics of any culture arise from legitimate needs during that culture’s history. However, one group’s cultural values, in particular, have obfuscated the valid cultural traditions of people groups the world over via mass colonization: White Supremacy Culture.
As defined by DismantlingRacism.org,
White Supremacy Culture is the idea (ideology) that white people and the ideas, thoughts, beliefs, and actions of white people are superior to People of Color and their ideas, thoughts, beliefs, and actions.
White supremacy culture is reproduced by all the institutions of our society. In particular the media, the education system, western science (which played a major role in reinforcing the idea of race as a biological truth with the white race as the “ideal” top of the hierarchy), and the Christian church have played central roles in reproducing the idea of white supremacy (i.e. that white is “normal,” “better,” “smarter,” “holy” in contrast to Black and other People and Communities of Color.
White supremacy culture is an artificial, historically constructed culture which expresses, justifies and binds together the United States white supremacy system. It is the glue that binds together white-controlled institutions into systems and white-controlled systems into the global white supremacy system.
Dismantling Racism names the following fifteen characteristics of White Supremacy Culture. I will seek to describe each in brief and explain how White Supremacy Culture influences childism, though you will likely see the problem before I get there.
Perfectionism: Inadequacies matter more than competencies, mistakes reflect badly on the person rather than being seen as neutral opportunities for reflection and growth, and problems are more identifiable than strengths.
Sense of Urgency: Schedules are more important than people, decision-making and strategizing are rushed, and results are more important than the process.
Defensiveness: Saving face and not ruffling any feathers get prioritized, hierarchies control for perceived insubordination, and leaders reject constructive feedback as unjust criticism.
Valuing Quantity over Quality: Meeting measurable goals takes precedence, emotions have no place, and completing the checklist wins out over any harm or the actual outcome.
Worship of the written word: Documenting everything accurately is more trusted than putting faith in people, and alternative communication styles are abhorred.
Belief in Only One Right Way: Divining the perfect solution to a problem is the goal and no flexibility exists to apply a fundamentally good solution in ways that address differences.
Paternalism: Only people in power are capable of making the right decisions for the people they rule and little vertical collaboration in the hierarchy occurs.
Either/or Thinking: Binary thinking rules, all nuance is lost, and the agenda of people in power gets advanced.
Power Hoarding: Preserving power toward the top of the hierarchy is key and those not in power are viewed as incompetent and emotional when they defy the power structure.
Fear of Open Conflict: Politeness rules all, conflict is unbearable, and emotional responses signal lack of intelligence or capacity.
Individualism: The ability of the individual is valued over the ability to work as a team, people should solve problems on their own, individuals want credit rather than cooperation, a rampant lack of accountability for those in power exists, and everyone is pushed into isolation as a result.
I’m the Only One Who Can Do This Right: The focus is on concentrating knowledge and effort into individuals, others cannot be trusted to do the thing correctly
Progress is Bigger and More: Progress matters more than process and those lacking power are exploited and excluded.
Objectivity: Neutrality is the priority, emotions invalidate the emotional person, perceived illogical thinking is met with impatience, and out of the box thinking is discouraged.
Claiming a Right to Comfort: Comfort for those in power is emphasized, those who cause discomfort get blamed, and fragility is the result.
Tema Okun, author and social justice advocate explains further that “the characteristics listed [above] are damaging because they are used as norms and standards without being proactively named or chosen by the group. They are damaging because they promote white supremacy thinking. Because we all live in a white supremacy culture, these characteristics show up in the attitudes and behaviors of all of us – people of color and white people.”
We are all influenced. Our worldviews are impacted. And, the way we approach parenting is affected. Here are a few of the ways in which White Supremacy Culture is impacting the way we treat our children.
Signs You’re Buying Into White Supremacy
At this point, your chest might be tightening a little. You might already be convincing yourself of how wrong I am. You couldn’t possibly be buying into White Supremacy Culture! Could you? Let me me the first one to admit that I struggle. I truly struggle. I see clearly where White Supremacy Culture has molded my thinking, even as a Peaceful Parent. The truth is that acknowledging reality and being honest with myself is the only way forward. Not only is it a way to become a better parent, for me, it’s also a way to help me become a better, more responsible white person.
I invite you to read through this list and see if your parenting has also been influenced by White Supremacy Culture like mine has.
Children can’t make mistakes without being punished
They are pulled to and fro by the draw of our schedules
We become incensed when our kids “disobey”
If our children aren’t progressing then they must be falling behind
Preliterate children in particular are infantilized by our communication requirements
We push kids toward the “right” way to do things and ignore their unique ideas
Children have no say in their upbringing
Children are either good or bad
Parents hold 100% of the power in the relationship
We demand politeness over realness
We expect our kids to figure things out on their own (“I’ve told you a hundred times! Go figure it out!”)
We react to mistakes by taking over
We praise progress and criticize mistakes made during the process
We believe we are more objective because we are less emotional than children
We punish children for “embarrassing” us in public
In the beginning of this piece, I looked at the ways in which cultures perceive time to illustrate the legitimate differences that exist across cultures. I talked about White Supremacy Culture and how ubiquitous it is. We are impacted by it without knowing it. I laid out the characteristics of White Supremacy Culture, followed by some of the ways in which White Supremacy Culture affects our children. If we accept that White Supremacy Culture does not contain exclusive knowledge of the only right way to believe and behave, what does that say about the way we treat children as isolated subordinates under the influence of white supremacy?
In 2013, Ghanian researcher, Patricia Mawusi Amos, authored a chapter in a book called Parenting in South American and African Contexts. Her chapter, Parenting and Culture – Evidence from Some African Communities, highlights common parenting practices in Ghana, Nigeria, and Liberia that produce positive results in children. Notably, she includes the extended family system, folktales, and puberty rites. These practices defy the White Supremacy Culture values of Paternalism, as multiple family and community members help care for the children; Sense of Urgency, as time is taken to teach children through storytelling; and Individualism, as children are included in cultural rites of passage.
And, research backs it up. For instance, Tadesse Jaleta Jirata’s 2014 paper, Positive Parenting: An Ethnographic Study of Storytelling for Socialization of Children in Ethiopia, concludes that the tradition of intergenerational storytelling “is a means for parents to accomplish their parenting responsibilities in line with the needs and concerns of their children,” “fosters close social relationships between parents and children and facilitates intergenerational transmission of knowledge and values,” builds “creative child-to-child interactions and help[s] children adapt themselves to their social world.”
So, if you find yourself locked into a White Supremacy Culture mindset, try moving in another direction. Read up on how parenting happens in other cultures. Look to find ways in which you can reduce the childism inherent in White Supremacy Culture. At this point, I should note that simply by engaging in Peaceful Parenting, you’ve already begun the work. One of the most common criticisms I’ve received about Peaceful Parenting is the amount of time it takes to go the gentle route. So, you know what? Go the gentle route! Ready for a final list?
How to Make a Positive Change
It’s one thing to say we want to reject White Supremacy Culture and quite another to actually do it. It’s hard to go against the grain. How about starting with a few resolutions to incorporate into your daily life?
Let children make mistakes without judgment. Check out this really cool research on how allowing people to self-correct their behavior builds executive function.
Slow down and be more choosy about the activities your family will engage in. Psychology Today has a great piece on how to do just that.
Find out how you can support your child’s communication through all stages of development from ZERO TO THREE, a global organization powered by leading researchers and clinicians.
Stop railing against “giving in” to your children and trying giving choices instead. Children who learn early how to make wise choices are better prepared for a lifetime of decision-making.
Understand that people are too complicated to be either good or bad. We are a culmination of all our experiences and all our reflections. Children benefit from being guided toward wisdom rather than being held to the impossible standard of “good.”
Recognize that kids don’t just choose not to do what we ask of them. Their executive function is developing and they need our help to figure things out. Check out this great overview for more details.
Recognize that you are not an objective observer removed from your relationship with your child. Both you and your child have human emotions that should be validated, not shunned.
I know this was a tough post to read. Did it help you see something you didn’t see before? Do you have a game plan for how you’d like to move forward with your new (or renewed) knowledge?
ABA is an extremely sensitive topic. You may experience intense emotions as you read this piece. I ask that you read through the post in its entirety before you make a final decision on what your perspective will be. If you need clarification, please ask. If you disagree, I’d appreciate your feedback.
It has taken me months to prepare this post for so many reasons, not the least of which is that I’ve been coming to terms with my own very late autism diagnosis. I’m one of the fortunate people who wasn’t subjected to Applied Behavior Analysis (ABA) therapy, but so many Autistic people are not so lucky. I write this post for them and for all the children now and in the future who will undergo this very painful experience.
At the start, I have to make clear that I am not a professional. I’m an Autistic mom of an Autistic child, and I have been in the position of deciding whether or not to put my child into ABA therapy.
I also need my fellow parents to know that I am not condemning you if you’ve chosen ABA therapy. It is the gold standard “treatment” for Autism Spectrum Disorder (ASD), it’s covered by insurance, and it certainly seems to work. Unless you’ve been exposed to Autistic adults and our position on ABA, there’s little reason for you to be concerned. I hope you will hear what we have to say and consider whether you want to continue down this path.
Autism Isn’t a Behavior Disorder
So, why treat it with compliance-based training? Autism is a completely natural, neurological variant. It is primarily disabling in cultures where Autistic people are not included and embraced.
Autistic brains perceive and process the world differently from allistic brains. But, we are fundamentally human beings, like everyone else, with the same emotions and responses to stimuli. If you hear a loud noise, do you not cover your ears? That’s not considered odd at all, right? So, why would it be odd for an Autistic person to do the same? Sure, it might be accompanied by humming and rocking, because stimming is so comforting to us, but we’re doing the same thing you do to reduce the strain of overstimulation. When allistic children relieve intense stress by cutting, we don’t send them to compliance-based training to try and coerce them to stop. We get them into helpful therapies to give them back control and provide relief that doesn’t harm, thereby addressing the problem rather than the behavior. And, that’s what Autistic kids need: acknowledgement that behavior is communication and relief from the underlying problem.
A History of ABA Therapy
Back in the 1970s, UCLA psychologist, Ole Ivar Lovaas, participated in the development of a therapy that promised to alter “deviant” behavior. His involvement in the Feminine Boy Project offered him an opportunity to engage in a form of behaviorism soon-to-be-called conversion therapy wherein gay men would theoretically be converted to heterosexuality. He also used this new therapy in his work with Autistic children.
Conversion therapy for homosexual people has since fallen out of favor, for obvious and good reason. However, Autistic children are still subjected to the same behaviorism that we’ve deemed unacceptable for use on other human beings. The reason? It was the same back then as it is now. In the words of Lovaas himself, ABA therapy can make Autistic kids “indistinguishable from their normal friends.” Unfortunately, that so-called progress comes at the price of an uptick in PTSD and suicide among Autistic people. I’m sure you can understand how devastating it is to go through life feeling that the person you genuinely are simply isn’t enough for the people who say they love you. Now, before you decide that my criticism is unfounded, let me make it abundantly clear that Lovaas was a pretty despicablefellow:
Modern ABA might look gentler on the surface; however, at its core, it starts with the assumption that Autistic people are broken and wrong, and it seeks to make our behavior more comfortable for allistic people.
Autistic Perspectives on ABA
Amythest Schaber is an Autistic artist, writer, public speaker, and advocate. Her series, Ask an Autistic, tackles a great many topics that have proved helpful to her many allistic followers. In this episode, she explains what ABA is from her perspective.
The following list includes links to other Autistic writers and advocates, as well as allies, who explain why ABA should be avoided:
Even new, “gentle” ABA therapy is problematic. (Source, source, and source)
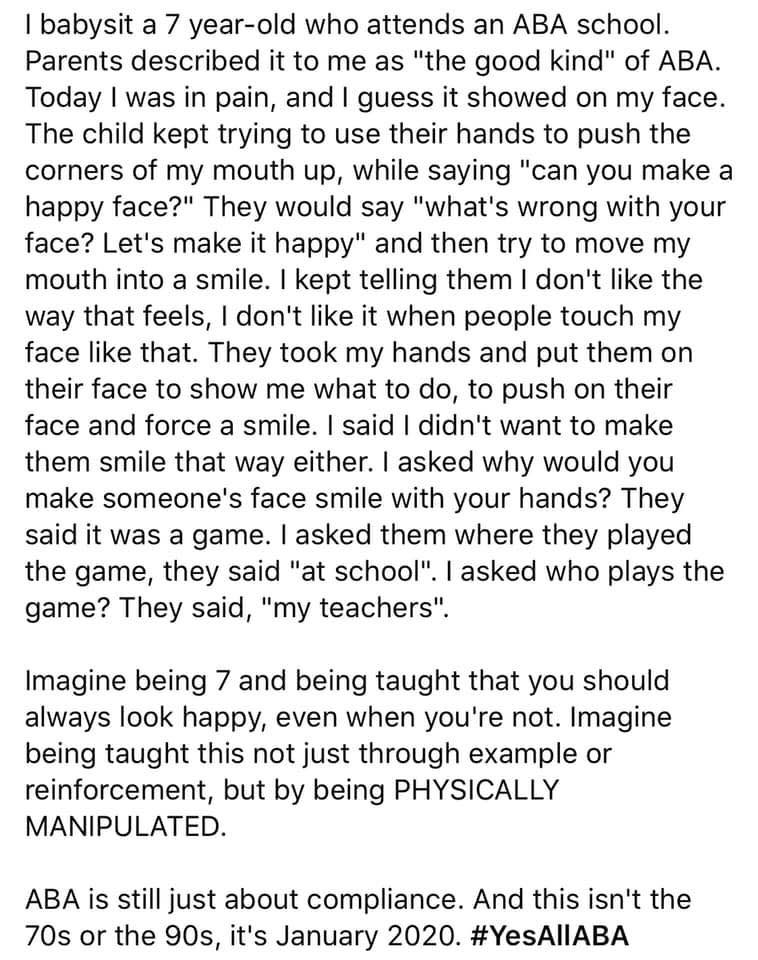
Finally, this post from the Non-Binary Intersectionalist (and I must give tremendous credit to this page for the wealth of resources I’ve been able to provide in this post!) describes a recent interaction with a young child in ABA therapy:
If you’re interested in reading some personal accounts of ABA therapy, I encourage you to check out this post on Stop ABA, Support Autistics. If you still aren’t convinced that ABA therapy is harmful, read this post.
What’s the Alternative to ABA Therapy?
To answer this question, we have to consider what well-meaning parents intend to happen when they put their children into ABA therapy. Some of the most common reasons I’ve seen are 1) to help the child be more independent, 2) to help the child navigate society more easily, and 3) to protect the child from danger. There are many, many more reasons of course! These are simply the top three as I’ve understood them.
I imagine you won’t be very surprised to learn that the best alternative to ABA therapy, in my experience and in accordance with my values, is Peaceful Parenting.
Peaceful Parenting achieves each of the three aims I mentioned by instilling self-sufficiency, self-assurance, and boundary recognition in children, as well as improving emotional development and self-regulation, one interaction at a time. Peaceful Parenting does not require thousands upon thousands of dollars or 40+ hours a week of therapy. For symptomatic concerns, there are other wonderful therapies like speech therapy, occupational therapy, and physical therapy. These therapies can help discover and meet needs that parents may not fully understand. And, much like taking an ESL class, they help Autistic kids learn a different culture without coercion.
Autistic kids deserve the same gentle treatment as any other child. If you wouldn’t put your neurotypical child into ABA therapy, there’s no need to put your Autistic child into ABA therapy. If you’d consider Dialectical Behavior Therapy (sidenote: DBT and ABA are not the same) to help your neurotypical child handle the stresses of life, offer the same to your Autistic child. Figuring out how best to support a child – any child – can be complicated. But treating our children with the same responsive gentleness, regardless of neurology, need not be the least bit complicated.
In this TED Talk, Dr. Amy Laurent explains why Autistic people need support in developing emotional skills, not behavior management:
ABA therapy is simply incompatible with Peaceful Parenting. The entire concept hinges on the adult therapist’s ability to coerce a child into compliance by withholding beloved objects and activities until the child “earns” them by obeying the therapist. ABA therapy discourages children from saying “no.” It does nothing to meet underlying, unmet needs and, instead, attempts to force children to ignore those needs while behaving as though the needs do not exist.
If you are a Peaceful Parent who is alarmed by what you’ve read, please know you and your child are enough just as you are. Your connection with your child is the key to comfort and growth. All children want to be heard and understood. Your job, then, is to learn how your child communicates and become conversant in their preferred language. Trust yourself. Trust your child. And, when you need help, find people who are willing to do the hard work of figuring out why your child is suffering and then find ways to relieve that suffering by way of accommodations and modifications. For instance, if your child hits himself in the head in the presence of very bright lights, the remedy is simple. Turn the lights down or off. When you start to see remedies everywhere, the rest falls right into place.
No Autistic child is the same and there are going to be things your child can do that mine can’t. Again, all Autistic people are different from one another. The key is learning what exactly that means for your child and filling in every single crevice in your child’s heart that is aching for your love and attention.
That includes Autistic children who exhibit self-destructive and violent behavior. Remember, all behavior is communication. If a child, any child, is lashing out, something is wrong that the child can’t overcome. Our goal as parents has to be to investigate the underlying cause of our children’s challenging behavior and help to relieve any stressors we discover.
You Want Action Steps? We’ve Got Actions Steps.
You’ll find this to be a very short section, because I’m directing you to the single most helpful post I’ve ever read on helping Autistic kids as a parent. For concrete, comprehensive details on what you can do for your Autistic child without the use of any ABA whatsoever, please read If Not ABA, Then What at The Thinking Person’s Guide to Autism. The recommendations there will support what you are already doing as a Peaceful Parent.
Careful! ABA Ideology Can Wriggle Into Other Therapies
If you’ve gotten this far, I want to make sure you know that ABA ideology has infiltrated all aspects of the way professionals care for Autistic people. Plus, because ABA is so profitable, some professionals use ABA codes to bill insurance even while they claim they aren’t practicing “traditional” ABA. However, don’t be fooled! If it’s called ABA, it is ABA. And, even if it’s not called ABA, the professional could be using ABA tactics to pressure your child into making advances. It can all be very confusing. An excellent post by Autistic Mama describes the red flags that should send you running for the door if you see them in any therapy your child undergoes. Please visit her post directly for a full explanation of each red flag.
Observation is Not Allowed
Indefinite Therapy
Extreme Hours
No Stimming Allowed
Requires Eye Contact
Excessive Reliance on Token Systems and Edibles
Rigid Approach or Refusing to Make Basic Accommodations
Focus on Outward Behaviors, Rather than Functional Skills
Expecting Kids to Perform on Command, Regardless of How Difficult Something is or Where the Child is at Emotionally
Moving too Fast or Not Breaking Down Tasks into Manageable Pieces
Learned Skills Don’t Transfer
Focus on Compliance
Focus on Verbal Communication
Punishment of Any Kind
Presumes Incompetence
You Are a Good Parent
Any parent who would go to the ends of the Earth, at any expense, for their child has earned that title. Please know my intention is not to attack you, though I understand why such an impact could result. You may be thinking that your child’s ABA looks nothing like what I’ve described or that your child loves their ABA therapist. I’m not here to argue or to condemn you. I ask only that you carefully consider the history of ABA, its inherent weaknesses, and the voices of Autistic adults urging caution.
A Thank You to All My Fellow Autistic Adults
This post wouldn’t have been possible without the labor of my fellow Autistics. You are so incredibly valuable and I appreciate you more than I can express. Thank you!
And, reader, thank you for listening.
Update (February 10, 2020): After I published this piece, it came to my attention that Alfie Kohn recently published an outstanding piece regarding new research into ABA. It’s well worth a read!
Disclaimer: Nothing stated in this post should be construed as an alternative to diagnosis and treatment by a medical professional. I am not qualified to provide medical advice.
If you’re anything like me, you’ve heard of the near miraculous wonders of melatonin supplementation. You may have also heard some of the not so great effects. So, let’s get down to the truth with our dear friend, science.
Use the Navigation links below to jump to sections of interest or read through for all the knowledge.
Melatonin (5-methoxy-N-acetyltryptamine) is a fat-soluble hormone that confers widespread health benefits and is produced in the pineal gland of the brain as well as by the retina of the eye and by the gastrointestinal tract. Production of endogenous (meaning made by the body) melatonin is triggered by darkness, and it typically peaks between 11 PM and 3 AM. Our bodies’ ability to produce melatonin decreases with age.
Melatonin “plays the role of a universal endogenous synchronizer” which, in addition to helping to maintain the wake-sleep cycle, also influences hemostasis, glucose homeostasis, phosphocalcic metabolism, blood pressure, and antioxidant defenses. In other words, melatonin stabilizes the circadian rhythms in the body, thereby impacting the body’s ability to coagulate blood, maintain normal blood glucose levels and blood pressure, metabolize phosphate and calcium for functions such as bone mineralization, and defend against the damage caused by free radicals.
Exogenous (meaning man-made) melatonin supplements can be made one of two ways. Either from the pineal glands of animals, which can be dangerous due to the potential for viral contamination, or as a synthetic product that is manufactured in a lab. Most commercial supplements are synthetic. Plant-based supplements are in the pipeline and melatonin naturally exists in the foods we eat as forms of it are produced by living organisms from animals to bacteria to algae to plants and beyond.
Back in 1994, Dr. Richard Wurtman, professor of neuroscience at MIT, led a team that confirmed where melatonin was produced in the body and how it functioned. His team discovered that a dose of 0.3 milligrams of melatonin helped older adults fall asleep faster and get back to sleep if they woke up in the night. However, researchers also discovered that commercial melatonin contained 10 times the effective dose, which, when taken regularly, ultimately overwhelms melatonin receptors in the brain, causing them to become unresponsive. At the time, he warned that “People should not self-medicate with melatonin.”
Studies to date have utilized pharmaceutical grade melatonin that is strictly regulated and certified to contain the ingredients in the appropriate proportions as labeled. Under these controlled conditions, substantive support exists for the presence of a plateau effect in adults with doses higher than 0.3 milligrams; the maximum effect being achieved at low doses with decreasing effectiveness in doses exceeding 1 milligram. In addition, there is some evidence that exogenous melatonin requires dosage over the course of a few days to achieve detectible effectiveness, and that it may increase in effectiveness over the course of time until the benefits plateau. The half-life of melatonin is less than one hour, which means that its usefulness from a given dose is short-lived. Some pharmaceutical grade melatonin medications have extended-release formulations to help improve the usefulness of the drug. It is unclear whether or not single doses of melatonin are effective.
High doses of exogenous melatonin have been demonstrated to desensitize receptors in the brain, thereby eventually making supplementation ineffective. However, without clear guidelines on appropriate dosing, the level at which overdose occurs remains unknown. Unfortunately, a 2017 analysis out of Canada found egregious mislabeling of melatonin supplements with counts varying from −83% to +478% of labeled melatonin. Chewable tablets suffered from the highest variability with one tablet containing nearly 9 milligrams of melatonin when it was labeled as 1.5 milligrams. Capsules suffered the greatest variability among lots. And, liquids had the greatest levels of stability, though they too were highly inconsistent. Oral and sublingual tablets with few ingredients proved the least variable of all the options. However, many of the supplements also contained impurities, including serotonin which has known effects and should not be taken by accident.
There is no known safe dose or dosing frequency for children.
Clinical Guidelines
In 2017, a task force from the American Academy of Sleep Medicine conducted a systematic review of the available literature to identify randomized controlled trials. Based on the evidence, this task force established recommendations for use by medical professionals. The task force listed 14 types of sleep aids and noted whether they were recommended for use or not. They advised clinicians not to use melatonin as a treatment for sleep onset and sleep maintenance insomnia.
Also, it is unknown whether melatonin supplements are safe during pregnancy or breastfeeding. High doses of melatonin may present fertility problems by affecting ovulation.
Possible Safety Issues
In 2015, Dr. David Kennaway conducted a review of the evidence for melatonin use in children, which was published in the Australian Journal of Paediatrics and Child Health. He determined that melatonin can produce “small advances in the timing of sleep onset” in both adults and children, but that there have “no appropriate studies to show that melatonin is safe in the long term for children or adults.” Use in children is always an off-label application of this hormone. He noted that, as a hormone, melatonin directly impacts the endocrine system and that long-term use may result in future “endocrine or other abnormalities.” He recommended that melatonin be prescribed only following a “biochemical diagnosis of an underlying sleep timing abnormality and after full disclosure to the carers of information about the known actions of melatonin on reproductive and other systems.”
In the United Stated, melatonin is considered a supplement. Therefore, it is generally unregulated by the Food and Drug Administration (FDA) and consumers have no guarantees regarding the safety of the commercial melatonin they purchase.
The Studies
When I began to seek out studies, I discovered thousands of papers that mentioned the term “melatonin.” In order to refine the list, I began by excluding studies published before 2009 and including only studies conducted on humans and written in/translated into English. From this list, I sorted by relevance and chose 175 to skim for abstracts. Then, I selected 80 to read in full, which resulted in a final resource list of 23 papers having targeted relevance. These studies involve research in countries around the world. I have grouped them by year for ease in assessing the progression of the research and recommendations.
2009
The effect of prolonged-release melatonin on sleep measures and psychomotor performance in elderly patients with insomnia https://www.ncbi.nlm.nih.gov/pubmed/19584739 doi: 10.1097/YIC.0b013e32832e9b08
OBJECTIVE: To investigate the effects of prolonged-release melatonin 2 mg (PRM) on sleep and subsequent daytime psychomotor performance in patients aged 55 years and older with primary insomnia.
FINDINGS: By the end of the double-blind treatment, the PRM group had significantly shorter sleep onset latency and scored significantly better on a psychomotor performance test than the placebo group.
2011
Melatonin for disordered sleep in individuals with autism spectrum disorders: systematic review and discussion https://www.ncbi.nlm.nih.gov/pubmed/21393033 doi: 10.1016/j.smrv.2011.02.001
OBJECTIVE: To provide a systematic review of efficacy and safety of exogenous melatonin for treating disordered sleep in individuals with ASD.
FINDINGS: The literature supports the existence of a beneficial effect of melatonin on sleep in individuals with ASD, with only few and minor side effects. However, these conclusions cannot yet be regarded as evidence-based. Randomized controlled trials and long-term follow-up data are still lacking.
Prolonged release melatonin in the treatment of primary insomnia: evaluation of the age cut-off for short- and long-term response https://www.ncbi.nlm.nih.gov/pubmed/21091391 doi: 10.1185/03007995.2010.537317
OBJECTIVE: To evaluate the age cut-off from a previous study for response to PRM and the long-term maintenance of efficacy and safety by looking at the total cohort (age 18-80).
FINDINGS: At 3 weeks, significant differences in favor of PRM vs placebo were found for the 55-80 year population but not the 18-80 year cut-off which included younger patients. Other variables improved significantly with PRM in the 18-80 year population more so than in the 55-80 year age group. No withdrawal symptoms or rebound insomnia were detected.
2012
Melatonin for sleep in children with autism: a controlled trial examining dose, tolerability, and outcomes https://www.ncbi.nlm.nih.gov/pubmed/22160300 doi: 10.1007/s10803-011-1418-3
OBJECTIVE: To assess dose-response, tolerability, safety, feasibility of collecting actigraphy data, and ability of outcome measures to detect change during 14-week intervention on children aged 3-10 years with a clinical diagnosis of an autism spectrum disorder who were free of psychotropic medications and whose parents reported sleep onset delay of 30 minutes or longer on three or more nights per week.
FINDINGS: Researchers documented an improvement in sleep latency with melatonin treatment. Because the study criteria were designed to enroll children with sleep-onset delay, they could not definitively comment on the effects of melatonin on sleep duration or night wakings.
2014
Optimal dosages for melatonin supplementation therapy in older adults: a systematic review of current literature https://www.ncbi.nlm.nih.gov/pubmed/24802882 doi: 10.1007/s40266-014-0178-0
OBJECTIVE: To define the optimal dosage of exogenous melatonin administration in disorders related to altered melatonin levels in older adults aged 55 years and above by determining the dose-response effect of exogenous administered melatonin on endogenous levels.
FINDINGS: Based on a systematic review of 16 articles from 1980 to 2013, nine of which were randomized controlled trials, the best applicable dosage for melatonin for older adults still cannot be adequately determined, as endogenous melatonin levels are subject to altered pharmacokinetics and -dynamics. This causes the risk of prolonged and elevated endogenous melatonin levels after exogenous melatonin administration in older adults. The researchers advise the use of the lowest possible oral dose of immediate-release formulation melatonin to best mimic the normal physiological circadian rhythm of melatonin and to avoid prolonged, supra-physiological blood levels.
The effectiveness of melatonin for promoting healthy sleep: a rapid evidence assessment of the literature https://www.ncbi.nlm.nih.gov/pubmed/25380732 doi: 10.1186/1475-2891-13-106
OBJECTIVE: To critically assess the available peer-reviewed literature on the use of melatonin in military service members and in healthy subjects to determine whether melatonin might be useful in military populations.
FINDINGS: The use of melatonin by healthy adults shows promise to prevent phase shifts from jet lag and improvements in insomnia, but to a limited extent. For the initiation of sleep and sleep efficacy, the data cannot yet confirm a positive benefit.
Melatonin in children with autism spectrum disorders: endogenous and pharmacokinetic profiles in relation to sleep https://www.ncbi.nlm.nih.gov/pubmed/24752680 doi: 10.1007/s10803-014-2123-9
OBJECTIVE: To describe overnight endogenous and PK melatonin profiles in children aged 3-8 years with ASD participating in open-label trial of melatonin for sleep onset insomnia.
FINDINGS: In children with ASD and insomnia responsive to treatment with supplemental melatonin, evidence exists for normal endogenous melatonin profiles. Furthermore, despite a relatively short duration of action of supplemental melatonin, night wakings improved in most children with treatment. This raises the possibility that supplemental melatonin may be influencing sleep onset delay and night wakings by mechnanisms other than simply replacing melatonin.
2015
The effect of melatonin treatment on postural stability, muscle strength, and quality of life and sleep in postmenopausal women: a randomized controlled trial https://www.ncbi.nlm.nih.gov/pubmed/26424587 doi: 10.1186/s12937-015-0093-1
OBJECTIVE: To document the safety of melatonin in postmenopausal women given evidence from previous studies that suggests a protective role of melatonin against osteoporosis through an increase of bone mineral density.
FINDINGS: Melatonin in a daily dose of 1 or 3 mg is safe to use in postmenopausal women with osteopenia. There is no long term hangover effect causing a reduction in balance- and muscle function or quality of life. In women with poor quality of sleep, small doses of melatonin trended towards improving quality of sleep.
OBJECTIVE: To establish a consensus on the roles of melatonin in children and on treatment guidelines at a conference in Rome in 2014.
FINDINGS: So far, the best evidence for the indication of melatonin treatment in children is for insomnia caused by circadian rhythm sleep disorders. Because insomnia due to other situations and disorders, including bad sleep hygeine, ADHD/ADD, personality disorders and depression, can mimic insomnia caused by circadian rhythm sleep disorders, the diagnosis should only be made after careful clinical assessment and possibly measuring dim light melatonin onset (DLMO). Melatonin can be effective not only for primary sleep disorders but also for sleep disorders associated with several neurological conditions. Controlled studies on melatonin for sleep disturbance in children are needed since melatonin is very commonly prescribed in infants, children and adolescents, and there is a lack of certainty about dosing regimens. The dose of melatonin should be individualized according to multiple factors, including not only the severity and type of sleep problem, but also the associated neurological pathology.
OBJECTIVE: To provide a succinct summary to help inform clinical and research practices for children with developmental disabilities (i.e. children with unspecified developmental delays or cognitive impairments and specific disorders/syndromes including ASD, Smith-Magenis syndrom, Angleman’s syndrom, fragile X syndrom, Down syndrom, and Rett syndrome).
FINDINGS: Following a review of a number of studies and a meta-analysis by Braam and associates, researchers determined that melatonin treatment yields beneficial effects with minimal side effects. However, melatonin is not approved by the US Food an Drug Administration and no drug is approved for use in pediatric insomnia (as of the time of this study).
OBJECTIVE: To provide information on the documented actions and properties of melatonin outside its ability to alter sleep timing that have been widely ignored but which raise questions about the safety of its use in infants and adolescents.
FINDINGS: Melatonin is increasingly being prescribed off lable for children and adolescents for difficulty in initiating and maintaining sleep. There is extensive evidence from animal and human studies that melatonin acts on multiple physiological systems, including the reproductive, cardiovascula, immune, and metabolic systems. Long-term safety studies on children and adults are lacking. Prescription of melatonin to any child whether severely physically or neurologically disabled or developing normally should be considered only after the biochemical diagnosis of an underlying sleep timing abnormality and after full disclosure to the carers of information about the known actions of melatonin on reproductive and other systems and the disclosure that there is a lack of appropriate studies conducted on children. Should endocrine or other abnormalities appear in the future in children previously treated with melatonin, it will not be tenable to argue that were were surprised.
OBJECTIVE: To present and evaluate the literature concerning the possible adverse effects and safety of exogenous melatonin in humans and provide recommendations concerning the possible risks of melatonin use in specific patient groups.
FINDINGS: A substantial number of both animal and human studies document that short-term use of melatonin is safe, even in extreme doses. No studies indicate that exogenous melatonin possesses any serious adverse effects. Also, randomized clinical studies indicate that long-term administration only induces mild adverse effects comparable to placebo treatment. Due to a lack of human studies, pregnant and breastfeeding women should not take exogenous melatonin. Also, long-term safety of melatonin in children and adolescents requires further investigation.
Melatonin Supplementation for Children With Atopic Dermatitis and Sleep Disturbance: A Randomized Clinical Trial https://www.ncbi.nlm.nih.gov/pubmed/26569624 doi: 10.1001/jamapediatrics.2015.3092
OBJECTIVE: To evaluate the effectiveness of melatonin supplementation for improving the sleep disturbance and severity of disease in children with AD.
FINDINGS: Sleep-onset latency shortened by 21.4 minutes after melatonin treatment compared with after placebo. Melatonin supplementation is a safe and effective way to improve the sleep-onset latency and disease severity in children with AD.
OBJECTIVE: To assess the evidence base for the therapeutic effects of exogenous melatonin in treating primary sleep disorders.
FINDINGS: Results from the meta analysis showed the most convincing evidence for exogenous melatonin use was in reducing sleep onset latency in primary insomnia, delayed sleep phase syndrome, and regulating the sleep-wake patterns in blind patients compared with placebo.
OBJECTIVE: To quantify melatonin in 30 Canadian commercial supplements, comprising different brands and forms and screen supplements for the presence of serotonin.
FINDINGS: Melatonin content was found to range from -83% to +478% of the labeled content. Additionally, lot-to-lot variable within a particular product varied by as much as 465%. This variability did not appear to be correlated with manufacturer or product type. Furthermore, serotonin was identified in eight of the supplements at levels of 1 mg to 75 mg. Melatonin content did not meet label within a 10% margin of the label claim in more than 71% of supplements and an additional 26% were found to contain serotonin. It is important that clinicians and patients have confidence in the quality of supplements used in the treatment of sleep disorders. To address this, manufacturers require increased controls to ensure melatonin supplements meet both their label claim, and also are free from contaminants, such as serotonin.
OBJECTIVE: To explore the evidence for using exogenous melatonin in the treatment of sleep disorders, both primary and secondary, in children and adults.
FINDINGS: There is evidence for the efficacy of melatonin in the management of insomnia and some intrinsic disorders of circadian rhythm in adults and children as well as in reducing sleep onset latency in jet-lag and shift work disorder in adults. Melatonin is used routinely in the treatment of rapid-eye movement sleep-behaviour disorder despite limited trial evidence. Increasingly, dual melatonin receptor agonists are being trialed in a variety of sleep disorders. Long-term adverse effects are currently not fully identified.
OBJECTIVE: To discuss the normal sleep development and needs in children, and we will provide an overview of sleep disorders, based on the 3rd edition of the International Classification of Sleep Disorders [ICSD-3].
FINDINGS: Melatonin is an effective, safe, and well-tolerated agent, particularly in cases of sleep-initiation insomnia caused by circadian factors. Several placebo-controlled studies of melatonin in adults and children (in some studies, as young as 3 years of age) showed that melatonin administered at bedtime reduces sleep-onset latency time and increases total sleep time.
OBJECTIVE: To review pharmacological treatment options for children and adolescents with ASD, with emphasis on recently published studies since our previous published update. We focus on randomized double-blind placebo controlled (RDBPC) trials, with at least 10 subjects. We also discuss CAM treatment options used in children with ASD.
FINDINGS: In addition to its effect on sleep, a few RDBPC trials have shown that melatonin can improve communication, rigidity, and anxiety in children with ASD.
Pharmacological and non-pharmacological interventions for non-respiratory sleep disturbance in children with neurodisabilities: a systematic review https://www.ncbi.nlm.nih.gov/pubmed/30382936 doi: 10.3310/hta22600
OBJECTIVE: To assess the clinical effectiveness and safety of NHS-relevant pharmacological and non-pharmacological interventions to manage sleep disturbance in children and young people with NDs, who have non-respiratory sleep disturbance.
FINDINGS: It was not possible to draw conclusions about the effectiveness of non-pharmacological interventions for managing sleep disturbance, and although there was some benefit with melatonin the degree of benefit is uncertain. There is some evidence of benefit for melatonin compared with placebo, but the degree of benefit is uncertain. There are various types of non-pharmacological interventions for managing sleep disturbance; however, clinical and methodological heterogeneity, few RCTs, a lack of standardised outcome measures and risk of bias means that it is not possible to draw conclusions with regard to their effectiveness. Future work should include the development of a core outcome, further evaluation of the clinical effectiveness and cost-effectiveness of pharmacological and non-pharmacological interventions and research exploring the prevention of, and methods for identifying, sleep disturbance. Research mapping current practices and exploring families’ understanding of sleep disturbance and their experiences of obtaining help may facilitate service provision development.
OBJECTIVE: To summarize some of the current knowledge about the potential effects of exogenous melatonin on puberty
FINDINGS: This review suggests that the role of melatonin in sexual maturation and the timing of puberty is understudied in humans. The three human studies that have examined the question have done so as an ancillary research question in small samples of children and youth, some of whom had neurodevelopmental disorders. This limits the generalizability to the general population and is insufficient evidence to draw conclusions for patients with mental health and neurological disorders. Further experimental studies on the impact of melatonin on puberty, notably in non-seasonal mammals, and advances in the research about the intermediary processes between melatonin and kisspeptin activation, could ultimately inform us about the potential influence of exogenous melatonin on puberty.
The effects of melatonin administration on disease severity and sleep quality in children with atopic dermatitis: A randomized, double-blinded, placebo-controlled trial https://www.ncbi.nlm.nih.gov/pubmed/30160043 doi: 10.1111/pai.12978
OBJECTIVE: To determine the effects of melatonin administration on disease severity and sleep quality in children diagnosed with atopic dermatitis (AD).
FINDINGS: Following 6 weeks of intervention, melatonin supplementation significantly improved SCORAD index, serum total IgE levels, and CSHQ scores. Though melatonin had no significant impact on pruritus scores, high sensitivity C-reactive protein, sleep-onset latency, total sleep time, weight and BMI compared with placebo. Overall, melatonin supplementation had beneficial effects on disease severity, serum total IgE levels and CSHQ among children diagnosed with AD.
2019
Exogenous melatonin as a treatment for secondary sleep disorders: A systematic review and meta-analysis https://www.ncbi.nlm.nih.gov/pubmed/29908879 doi: 10.1016/j.yfrne.2018.06.004
OBJECTIVE: To determine the efficacy of exogenous melatonin versus placebo in managing secondary sleep disorders.
FINDINGS: Meta-analysis of the data from a series of studies with small sample size demonstrates that exogenous melatonin improves the sleep quality of secondary sleep disorders. Based on the current advantages of melatonin in the management of secondary sleep disorders, it is hoped that there will be a tremendous growth in the use of melatonin application worldwide. Besides, little evidence is available regarding the adverse effects of long-term use of melatonin. Clinicians should be alert to these shortcomings but also aware of the potential role of melatonin in clinical psychiatry and sleep medicine.
OBJECTIVE: To review the role of melatonin in the circadian regulation of sleep and mood and the phase-shifting and sleep-promoting properties of exogenous melatonin and melatonin agonists and outline how melatonin and melatonin agonists might be used for treatment of various sleep and mood disorders.
FINDINGS: The phase-shifting and sleep-promoting effects of melatonin plus additional effects of melatonin agonists on melatonin and serotonin receptors have shown promise for novel treatments for a variety of circadian, sleep and mood disorders. Importantly, the main advantage melatonin and its agonists offer over traditional sleep and depression treatments is that they assist to restore circadian function which is often misaligned in these disorders and which is increasingly thought to be a causal mechanism and part of the aetiology of sleep and mood disorders. Treatments that fail to address the misaligned circadian system present in sleep and mood disorders may not fully address the underlying causes, and for this reason, further investigation on the potential for melatonin-based treatments should be undertaken.
Assessment of the Evidence
Endogenous melatonin provides widespread health benefits for the human body across many functional systems. Exogenous melatonin is strongly evidenced as an effective sleep aid for sleep onset (meaning, falling asleep) and less strongly for night wakings and other other sleep-related applications in adults aged 55 and older.
However, the literature is glaringly lacking in randomized, controlled trials as well as research on younger adults, teenagers, adolescents, children, and infants. Existing studies utilize small subject pools and short- to medium-term time frames for research, most stopping short at 3 months and few-to-none lasting more than one year. There is no evidence yet that consistent long-term use is safe for any age group. Dosing remains a challenge and a standard dosing table does not yet exist, although it has been long established that overdoses cause receptors in the brain to become unresponsive and supplementation to be rendered useless. Given the lack of information about dosing, it is impossible to determine what amount constitutes an overdose without investigative blood work. Melatonin supplements are almost entirely unregulated in the United States, so high doses are regularly consumed. While high doses don’t appear to have extreme deleterious effects on humans, the fatal dose is yet unknown. Future studies are needed to ameliorate concerns about safety, dosage, and pediatric use.
Promoting Better Sleep
While I cannot make any formal recommendations to you about whether or not to give your child melatonin, I can suggest some solutions to help with sleep outside of melatonin supplements.
Eating lots of fresh fruits, vegetables, whole grains, and low fat protein sources provides plenty of tryptophan as well as group B vitamins, minerals, and unrefined carbohydrates, all of which supports healthy sleep. Reach for things like salmon, poultry, eggs, spinach, seeds, milk, soy products, and nuts to get a good dose of sleep-promoting nutrients. (Source and Source)
Tart Montmorency cherries contain high levels of phytochemicals including melatonin. Cherry juice is a natural source of plant-based exogenous melatonin and may help support good sleep. (Source)
Exercise in the mornings can improve the quality of nighttime sleep by “increasing parasympathetic nerve activity.” However, high-intensity exercise in the evening should be avoided. Getting your child out for some fresh air every morning may make your bedtime routine a breeze. (Source)
Common wisdom says to help your child avoid blue light LED sources like smartphones, tablets, and TVs near bedtime as this type of light may suppress endogenous melatonin. (Source) However, there is also evidence that such recommendations may be misguided. (Source) Use your best judgment as you watch how nighttime blue light stimulation impacts your child.
In one of the studies referenced in this Guide, a young girl did not respond to melatonin treatments but was later diagnosed with bipolar disorder, medicated with risperidone, and subsequently experienced improved sleep. If your child is really struggling, it may be worthwhile to seek out age-appropriate therapy to rule out other treatable sources of difficulty. (Source)
The Bottom Line
Do melatonin supplements help your child? Unless you’re using pharmaceutical grade supplements under the strict care of a physician, my best answer is maybe. But it’s hard to know what your child really needs in the way of a dose without extensive blood work . The placebo effect is also in play to an extent. If you and your child believe the supplement works, it’ll probably work even better than the actual physiological impact, if there is one to begin with.
Will melatonin supplements seriously harm your child? Probably not, but there’s no guarantee and there are other effective options that don’t involve using unregulated supplements with potentially harmful impurities.
If you discover any errors in my work, please contact me at peacefulmom(at)peaceigive.com.